11 april 2011
Therapietrouw bij schizofrenie verhogen
Dr. Tonnie Staring
GZ-psycholoog / gedragstherapeut VGCt
ABC voor jongeren met psychotische kwetsbaarheid
Altrecht
Leerdoelen
- Prevalentie en consequenties van
therapieontrouw kennen bij schizofrenie
- Ideeën ontwikkelen omtrent wat wel en niet
nuttig is bij het verbeteren van therapietrouw
- Deze ideeën kunnen aanpassen aan individuele
situaties en motieven van patiënten
Het is niet eenvoudig om therapietrouw te zijn
Keith et al., J Clin Psychiatry 2003; 64: 1308-1315
Prevalentie van ontrouw
CATIE: 74% van de patiënten stopte of switchte met de
antipsychotische medicatie binnen 18 maanden 1
Gemiddeld wordt slechts 58% van de antipsychotische
medicatie gebruikt 2
Therapietrouw wordt overschat door hulpverleners en zelfs
door de patiënten zelf 3
1 Thomas, Eur Neuropsychopharmacol. 2007; suppl 2: S115-22
2 Crames & Rosenheck, Psychiatric Services 1998; 49: 196-201
3 Byerly et al., Psychiatric Services 2007; 58: 844-847
Gevolgen van therapie-ontrouw bij schizofrenie
• Risico op terugval en heropname wordt 3 tot 5 maal hoger 1, 2, 3, 4, 5
• Als (1) 50% = ontrouw, (2) ratio heropname = *4 en (3) causaliteit
dan wordt 60% van de heropnames veroorzaakt door therapie-ontrouw
• Risico op suïcide ligt 3,75 maal hoger 6
• Dakloosheid, detentie en geweld 7
1 Dixon & Lehman, Schizophr Bulletin 1995; 21: 631-743
2 Fenton et al., Schizophr Bulletin 1997; 23: 637-651
3 Robinson et al., Schizophr Research 2002; 57: 209-219
4 Ucok et al., Europ Arch Psych and Clin Practice 2006; 256: 37-43
5 Weiden et al., Psychiatric Services 2004; 55: 886-891
6 Hawton et al., BJP 2005; 86: 9-28
7 Torrey & Zdanowics, Psychiatric Services 2001; 52: 337-341
Interventies
• Moderne antipsychotica geen hogere compliance 1
• Depot werkt voor een deel 2
• Psycho-educatie werkt niet op therapietrouw 3, 4, 5
• Compliance Therapy werkt matig tot niet 6, 7, 8, 9
• Visual Feedback Therapy werkt matig tot niet 10, 11
• Gedragstraining, medicatie aan doelen/waarden
1 Voruganti et al., Curr Opin Psychiatry 2008; 21: 133-139
van patiënt koppelen lijkt te werken 3
2 Kane CNS Spectr 2006; 11 (12 suppl 14): 1-7
3 Zygmunt et al., Am J Psychiatry 2002; 159: 165-64
4 Dolder et al., J Clin Pharmacology 2003; 23: 389-99
5 Lincoln et al., Schiz Research 2007; 96: 232-245
6 O’Donnel et al., BMJ 2003; 327: 834-6
7 Byerly et al., J Clin Psychiatry 2005; 66: 997-1001
8 Kemp et al., BJP 1998; 172: 413-419
9 Gray et al., BJP 2006; 189: 508-514
10 Kuzoki et al., Arch Psychiatr Nurs 2005; 19: 70-80
11 Cramer & Rosenheck, J Nerv Ment Dis 1999; 187: 53-5
Heterogene oorzaken van ontrouw?
Plenair brainstormen
Casuïstiek?
Iemand eigen casus om in te brengen?
Ambulante casus 1
Ahmed heeft schizofrenie, gedesorganiseerde
type. Hij woont bij zijn ouders en probeert met
hulp structurele dagbesteding op te pakken. Hij
vindt antipsychotica nuttig, maar blijkt de pillen
bij navraag vaak te vergeten. Hij maakt zich hier
zorgen over, en de spanning die dat oplevert
doet de chaos in zijn hoofd toenemen, met als
gevolg dat hij er nog minder goed in slaagt om
de medicatie iedere dag te gebruiken.
Wat kun je voor Ahmed betekenen?
Ambulante casus 2
Evelien heeft schizofrenie, paranoïde type. Ze had
in het verleden veel last stemmen, maar dat is nu
sinds drie maanden verholpen middels risperdal.
Echter, Evelien klaagt over maagklachten en over
moeheid. Ze wijdt het stoppen van de stemmen
ook niet echt aan de medicatie, en vindt dat het
niet zo goed voor haar werkt. Ze vraagt daarom
de hele tijd of ze niet kan afbouwen of stoppen,
en je twijfelt aan haar huidige therapietrouw.
Wat kun je voor Evelien betekenen?
Ambulante casus 3
Consuelo heeft schizofrenie paranoïde type. Hoewel
ze al drie keer gedwongen werd opgenomen, en
telkens opknapte bij het instellen op antipsychotica,
is ze het niet eens met de diagnose en behandeling.
Ze wil de medicatie niet nemen, want dat zou voor
haar inhouden dat ze toegeeft dat ze gek is. Ze wil
juist dat mensen erkennen dat de buurtkinderen
haar echt lastigvallen, en dat haar ex-man haar echt
in de gaten heeft gehouden. Het gaat weer minder
goed met haar de laatste tijd, en ze geeft toe alweer
enige weken te zijn gestopt met antipsychotica.
Wat kun je voor Consuelo betekenen?
Ambulante casus 4
Adam heeft schizofrenie paranoïde type, en is ook
polydrugs-gebruiker. Hij zit wisselend op de kliniek, in
een beschermde woonvorm, of is dakloos. Hij heeft
geen inzicht en ervaart veel cognitieve problemen. Hij
accepteert zolang als zijn (voorwaardelijke) RM duurt de
depot-injectie van antipsychotica. Daarna stopt hij
telkens weer, met altijd een gedwongen opname als
gevolg. Hij verliest dan telkens alles dat men probeerde
op te bouwen: een dak boven zijn hoofd, dagbesteding,
de herstelde relaties met familieleden, etc. Er zijn veel
dingen geprobeerd om hem te motiveren en inzicht te
bieden, maar niks helpt. Op dit moment loopt de voorw.
RM weer af, en hij zegt weer te gaan stoppen met zijn
depot.
Wat kun je voor Adam betekenen?
In groepjes
Brainstormen over casuïstiek
Voor Ahmed, Evelien en Consuelo:
TAT
Treatment Adherence Therapy
TAT
Three clusters of patient-determinants of non-adherence 1
•
(A) Stigma, sealing-over recovery style, denial of illness, little insight, little hope
•
(B) Low efficacy and side-effects of medication / negatieve attitude towards
medication
•
(C) Cognitive deficits, little daily structure, lessened initiative
1 Staring ea, Current Psychiatry Reviews 2006; 2 (4): 487-494
Cause of non-adherence:
The patient denies or seals over
his illness; has not integrated
illness and treatment into life.
The patient is not satisfied
with the medication / low
efficacy or side-effects.
The patient lacks the
skills or structure to
effectively participate
with the treatment.
Non-adherence
Strategy:
Motivational
Interviewing
Medication
Optimization
Behavioral
Training
TAT 1
1 Staring ea, Current Psychiatry Reviews 2006; 2 (4): 487-494
TAT: the protocol
•
Assessment phase
•
Module 1: Behavioral Training
•
Module 2: Medication Optimization
•
Module 3: Adapted Motivational Interviewing
•
Booster sessions
About six months of treatment
TAT: Assessment phase
•
Normalization of non-adherence
•
Non-judgmental way of asking
•
Inventory of (cultural) illness-beliefs, insight, recovery style,
experienced stigma, medication attitude, efficacy, side-effects,
personal experiences with mental health institutions
TAT: Behavioral Training
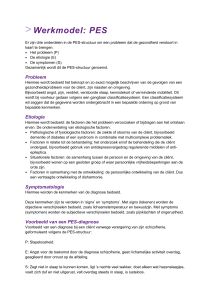
TAT: Medication Optimization
TAT: Medication Optimization
Week
1
Medication
none
voices
sexually explicit images
arguing with the voices
being physically influenced
Dosage
Rating:
7
10
7
7
•
Symptoms:
-
•
Side-effects:
- feeling like a zomby
- drousiness
0
0
•
General:
- doing fun things
- general feeling
3
4
TAT: Adapted Motivational Interviewing
TAT: Adapted Motivational Interviewing
Added elements
- Destigmatizing strategy: illness normalization
- Destigmatizing strategy: discussing famous people
- Education with the stress-vulnerability model
- Adaptations for negative symptoms & cognitive
impairments
Motivational Interviewing: the core
Discrepancy
Experienced friction between
behaviour and goals / values
+
Self-efficacy
=
The basis
Basic principles
Basic techniques
- Express empathy
- Open questions
- Ambivalence is normal
- Reflective listening
- Roll with resistance
- Summarize
- Support self-efficacy
- Affirm
- Elicit change talk
Resistance and change talk
Minimize resistance
Optimize change talk
- Reflections
- Ask straight out
- Emphasize autonomy
- Query extremes
- Shift focus
- Elaborate
- Looking back and forward
- Explore goals and values
- Confidence ruler
Estimate behaviour
consequences
Experience stress
and friction
Apathy
Cognitive biases
(JTC, BM, CB, etc.)
Disorganization
Discrepancy
Poverty of speach
Experienced friction between
behaviour and goals / values
Self-efficacy
Poor executive
functioning
Experience pride
and confidence
Stigma
Imagine a plan
Connect past
successes
Overgeneral memory
Connect past
experiences
Have goals
and values
Overview
information
White = the goal
Yellow = needed
Red = some barriers
Adaptations of Motivational Interviewing
in patients with psychotic disorders
- Patience
- Negative symptoms: are they always that?
- The therapist is more active
- Disorganization and lengthy aimless speach: use fewer open questions
- Visual support
- Reflections also serve to maintain the logical structure of the conversation
- Decisional balance in just two colums
- More affirming, acknowledgement and stressing personal autonomy
- Pause sometimes
- More psycho-education
Kemp & David, Br J Psych 1995; 54: 222-7
Martino et al., J Subst Ab Tr 2002; 23: 297-308
Rusch & Corrigan, Psych Reh J 2002; 26: 23-32
Treatment Adherence Therapy
Randomized Controlled Trial
Target patient group
Outpatients
Schizophrenia or schizoaffective disorder (CIDI)
Mastery of the Dutch language
Problems with service engagement (SES)
Progression through the trial
Assessed for eligibility
(n=391)
- Did not meet inclusion
criteria (n=196)
- Refused to participate
(n=79)
Received baseline
assessment (n=116)
Randomized (n=109)
TAU (n=55)
TAU + TAT (n=54)
Refused further
participation (n=7)
Progression through the trial
TAU (n=55)
Received TAU (n=54)
Lost to 6-month assessment
- died (n=1)
- refused interview (n=1)
- stopped all treatment (n=1)
TAU + TAT (n=54)
Received TAT (n=47)
Discontinued TAT (n=6)
Lost to 6-month assessment
- dropped out of study (n=1)
Lost to 12-month assessment
- died (n=2)
- stopped all treatment (n=1)
Lost to 12-month assessment
- dropped out of study (n=1)
Primary outcome analysed
- with 6-month data (n=52)
- With 12-month data (n=52)
Primary outcome analysed
- with 6-month data (n=53)
- With 12-month data (n=53)
Results
Effects on service engagement
MANCOVA:
T1
F = 9.75
Sig = .002
T2
F = 4.64
Sig = .023
Effects on medication compliance
MANCOVA:
T1
F = 11.77
Sig = .001
T2
F = 4.73
Sig = .032
Effects on re-admissions
Cumulative percentage of patients admitted
TAT group
Control group
30
25
20
15
10
5
0
T0
T1
T2
Effects on involuntary re-admissions
Cumulative percentage of patients involuntarily admitted
TAT group
Control group
14
12
10
8
6
4
2
0
T0
Fisher’s Exact test: Sig = .053
T1
T2
Effects on other secondary outcomes
PANSS positive symptoms:
No effects
PANSS negative symptoms:
No effects
PANSS general pathology:
No effects
Quality of life (EQ-5D):
No effects
Functioning (HoNOS):
No effects
Effects on mediators
Insight into illness (IS):
No effects
Experienced Stigma (SS):
No effects
Recovery Style (RSQ):
No effects
Therapeutic Alliance (WAI):
No effects
Self-esteem (SERS-SF):
No effects
Conclusions
There is considerable heterogeneity in patients’ reasons for
treatment non-adherence
When strategies are tailored to patients’ individual situations,
we can support treatment adherence (using TAT)
Despite the effects, symptoms and quality of life did not
improve
The mechanism of change is unclear
Limitations
Sample size was not very large
Attention was unevenly distributed between the two treatment
allocations
Measuring compliance is not easy
Strenghts
Well defined treatment protocol
Therapists in routine settings performed the interventions
Masked independent assessors of outcome
Relatively high inclusion and follow-up rates
Discussion - why did QOL not improve?
Psychotic symptoms
- 0.17
- 0.23
Medication
compliance
0.33
no association
Quality of life
0.22
Adverse
medication effects
- 0.48
Staring ea, Schizophrenia Research 2009; 113: 27-33
Discussion - why did symptoms not improve?
Other studies had similar findings 1,2
Invalid adherence measurements?
Small sample sizes?
Symptoms were relatively under control at baseline?
More intensive treatment was needed in the control group (admissions)?
Non-adherent patients: illness characteristics and poor treatment response?
Antipsychotic medications have an impact on behaviour, emotion, and preoccupation,
rather than on the conviction and external perspective of psychotic experiences 3
1 Kemp ea, British Medical Journal 1996; 312: 345-349
2 Velligan ea, Schizophrenia Bulletin 2008; 34: 438-493
3 Mizhari ea, Schizophrenia Research 2006; 88: 111-118
Voor Adam:
Iets anders?
Vragen we niet teveel?
Keuze
Tonnie
Staring
Patiënt met
schizofrenie
Negatief
gevolg
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
Vragen we niet teveel?
Keuze
Tonnie
Staring
Patiënt met
schizofrenie
Wel of niet
nog een
glas wijn?
Negatief
gevolg
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
Vragen we niet teveel?
Keuze
Tonnie
Staring
Patiënt met
schizofrenie
Negatief
gevolg
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
Vragen we niet teveel?
Keuze
Tonnie
Staring
Patiënt met
schizofrenie
Negatief
gevolg
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
Kans op
gevolg
100%
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
Vragen we niet teveel?
Keuze
Tonnie
Staring
Patiënt met
schizofrenie
Negatief
gevolg
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
Kans op
gevolg
Duur
tot
gevolg
100%
8 uur
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
Vragen we niet teveel?
Keuze
Tonnie
Staring
Patiënt met
schizofrenie
Negatief
gevolg
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
100%
8 uur
Goed /
volledig
inzicht
Negatieve
sympt. en
‘willed
action’
Vragen we niet teveel?
Keuze
Tonnie
Staring
Patiënt met
schizofrenie
Negatief
gevolg
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
100%
8 uur
Goed /
volledig
inzicht
‘willed
action’
intact
Vragen we niet teveel?
Keuze
Negatief
gevolg
Tonnie
Staring
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
Patiënt met
schizofrenie
Wel of niet
pillen
nemen?
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
100%
8 uur
Goed /
volledig
inzicht
‘willed
action’
intact
Vragen we niet teveel?
Keuze
Negatief
gevolg
Tonnie
Staring
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
Patiënt met
schizofrenie
Wel of niet Psychose
pillen
en opname
nemen?
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
100%
8 uur
Goed /
volledig
inzicht
‘willed
action’
intact
Vragen we niet teveel?
Keuze
Negatief
gevolg
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
8 uur
Goed /
volledig
inzicht
‘willed
action’
intact
Tonnie
Staring
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
100%
Patiënt met
schizofrenie
Wel of niet Psychose
pillen
en opname
nemen?
4 * grotere
kans, maar
nog steeds
< 100% 1
1 Weiden et al., Psychiatr Serv 2004; 55: 886-891
Vragen we niet teveel?
Keuze
Negatief
gevolg
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
Goed /
volledig
inzicht
‘willed
action’
intact
Tonnie
Staring
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
100%
8 uur
Patiënt met
schizofrenie
Wel of niet Psychose
pillen
en opname
nemen?
4 * grotere
kans, maar
nog steeds
< 100% 1
0 – 2 jr
1 Weiden et al., Psychiatr Serv 2004; 55: 886-891
Vragen we niet teveel?
Keuze
Negatief
gevolg
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
‘willed
action’
intact
Tonnie
Staring
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
100%
8 uur
Goed /
volledig
inzicht
Patiënt met
schizofrenie
Wel of niet Psychose
pillen
en opname
nemen?
4 * grotere
kans, maar
nog steeds
< 100% 1
0 – 2 jr
Slecht /
beperkt
inzicht
1 Weiden et al., Psychiatr Serv 2004; 55: 886-891
Vragen we niet teveel?
Keuze
Negatief
gevolg
Kans op
gevolg
Duur
tot
gevolg
Cognitieve
capaciteit /
inzicht
Negatieve
sympt. en
‘willed
action’
Tonnie
Staring
Wel of niet Kater, kan
nog een
presentatie
glas wijn? niet volgen
100%
8 uur
Goed /
volledig
inzicht
‘willed
action’
intact
Patiënt met
schizofrenie
Wel of niet Psychose
pillen
en opname
nemen?
4 * grotere
kans, maar
nog steeds
< 100% 1
0 – 2 jr
Slecht /
beperkt
inzicht
‘willed
action’
beperkt,
meer cued 2
1 Weiden et al., Psychiatr Serv 2004; 55: 886-891
2 Langdon et al., Psychiatr Res 2007; 150: 193-197
Patiënten met geld belonen voor
therapietrouw?
Financiële beloning voor goed of gezond
gedrag is niet nieuw
•
Contingency Management bij drugsgebruik, meta-analyse bij 47 studies: 21%
gebruikte geld als beloning
•
Contingency Management voor AIDS medication adherence, mogelijke geldprijzen als
beloning
•
Geld bij DD voor abstinentie, behandeling volgen, en plannen maken
•
Geld voor verslaafde die zich steriliseert
•
Bonus voor artsen die patiënten van het roken afhelpen in Engeland
•
Geld voor file mijden bij Hollandse brug A6
Werkt geld betalen ook voor verhoging
therapietrouw bij schizofrenie?
Pilot in Nederland:
percentage van depot injecties geaccepteerd
1 jr voor m4m
1 jr tijdens m4m
100
90
80
70
60
50
40
30
20
10
0
patiënt A
patiënt B
patiënt C
patiënt D
patiënt E
Pilot in Nederland:
Aantal opnamedagen
1 jr voor m4m
1 jr tijdens m4m
300
250
200
150
100
50
0
patiënt A
patiënt B
patiënt C
patiënt D
patiënt E
Pilot in Engeland: aantal opnamedagen bij patiënten
met schizofrenie of verwante stoornis
2 jr alvorens betaling
400
Sinds betaling
350
300
250
200
150
100
50
0
patiënt A
patiënt B
patiënt C
patiënt D
Claassen et al., Psychiatr Bull 2007; 31: 4-7
En wat wanneer het betalen weer stopt?
Externe beloning lijkt de intrinsieke motivatie bij kinderen en studenten te
verminderen. 1 Wanneer beloning stopt: gedrag < baseline niveau?
(overjustification effect)
Dit is een lopend debat 2, 3
Contingency Management bij drugsgebruik had achteraf geen negatief effect
op de onderliggende motivatie. Langere abstinentie leek positief te werken
op motivatie. 4
1 Deci et al., Psychological Bulletin 1999; 125: 627-668
2 Reiss, Behavior-Analyst 2005; 28: 1-14
3 Cameron & Pierce, ‘Rewards and Intrinsic Motivation: Resolving the controversy’ 2002; Greenwood press
4 Ledgerwood & Petry, Drug and alcohol dependence 2006; 83: 65-72
Indien het werkt… Is het wel ethisch?
BMJ stelde de vraag aan professionals:
“Is it acceptable for people to be paid to adhere to medication?”
120
100
80
95
60
40
38
20
0
No
Yes
In Nederland zijn professionals op het eerste oog veel minder kritisch
Is het ethisch? – praktische zaken
• Hoeveel geld geef je?
• Wie betaalt het?
• Werkt het beter dan andere beloningen? (bonnen, voedsel, etc)
• Als ze er drugs van kopen, is er dan nog gezondheidswinst?
• Zal het overjustification-effect plaatsvinden?
• Raken voorheen gemotiveerde patiënten gedemotiveerd?
• Kan levenslange geld-beloning overwogen worden?
• Kun je het aan iedereen aanbieden?
• Worden hulpverleners er lui van?
Is het ethisch? – principiële zaken
• Vergelijking andere gebieden waar geldbeloning plaatsvindt
• Vergelijking andere dwang/drang methoden? (voorw RM, etc)
• Verhoogt / verlaagt het de autonomie van de patiënt?
• Incommensurabiliteits-argument?
• Oneerlijk voor andere patiënten?
• Mogen ze er iets mee doen waar hulpverlening eigenlijk niet
achter staat (drugs, etc)?
• Misbruik van zwakke patiënten voor verkeerde doeleinden?
Wat loopt er momenteel?
• Audier, Mulder, Staring, ea starten in Den Haag en omstreken een grote
trial m4m bij dubbele diagnose patiënten
• Priebe ea doen momenteel kwalitatief onderzoek naar de ethiek
• Priebe ea starten in Engeland met een grote trial m4m
11 april 2011
Dr. Tonnie Staring
GZ-psycholoog / gedragstherapeut VGCt
ABC, Altrecht
[email protected]