ESPEN Congress Lisbon 2004
Enteral nutrition and gut function
Feeding the patient/feeding the gut
Peter Soeters
Feeding the Gut
Department of Surgery
academic hospital Maastricht
The Relevance of intact
gutfunction
•
•
•
The Gut-Liver axis
Permeability and Translocation/MOF
Conclusions
Dagci et al Acta Tropica 2002 81:1-5
Rocha et al Surgery 2001 130:65-73
Rinsema et al
SGO 1988 167: 372-6
Rinsema et al
SGO 1988 167: 372-6
Spitz et al
Crit Care Med 1996 24: 635-41
Kyiama et al
JPEN 1998 22:
276-279
Capron et al
Lancet 1983 26: 446-7
Kwashiokor:
Undernutrition and Infection
Marasmus:
Undernutrition
Welsh et al
Gut 1998 42: 396-401
Perdue Mary Am J Phys 1999 G1-G5
Jejunal-ileal bypass!
Drenick et al
GE1982 82:535-48
Garcia-Lafuente et al Gut 2001 48:503-507
Garcia-Lafuente et al Gut 2001 48:503-507
Shi Qi Yang et al, ProcNatlAcadSci 1997; 94: 2557-2562
Shi Qi Yang et al, ProcNatlAcadSci
1997; 94: 2557-2562
Shi Qi Yang et al, ProcNatlAcadSci 1997; 94: 2557-2562
Shi Qi Yang et al, ProcNatlAcadSci 1997; 94: 2557-2562
Wigg et al, Gut 2001; 48:206-211
Wigg et al, Gut 2001; 48:206-211
Tilg and Diehl,
NEJM 2000;
343: 1467-1476
No food/intest.secretions in small
bowel
•
•
•
•
Intoxicates the liver
Refunctionalisation relieves the intoxication
Bile, gastric and pancreativ juice, and nutrition
Intrahepatic cholestasis is not exclusively dependent
on Parenteral Nutrition
• Morbidity, Mortality (especially in children)
• The non-functioning gut induces direct of indirect
toxic impulses, NASH and diminished immune
function of the liver (exp)
The Gut-Liver axis
•
•
•
•
•
•
No food, no secretions
Stasis of luminal contents/Stenosis
Bacterial overgrowth
Secondary bile acids (toxic for the liver)
Increased absorption of toxins
Inbalance of Pro- en Anti-inflammatory
Cytokines and direct consequences for
the liver
• Undernutrition/Depletion
• A diminished bile acid pool (less binding
of endotoxin?)
The TPN-Liver axis
•
•
•
•
•
Septic patients clear less fat
Clearance of Parenteral fat is worse than Enteral fat
Some fats are worse than others
Many patients have already steatotic livers
Hypertriglyceridemia/Steatosis and Cholestasis go
hand in hand
• These abnormalities cause liver failure in the long run
– liver transplantation in children
– Liver transplantation in patients with malabsorptive (bypass)
surgery for morbid obesity
– Liver failure in Short Bowel patients with home TPN
• Steatosis may depress immunefunction in the short
term and may sensitize the liver to endotoxin
Moore et al, Ann Surg 1992; 216: 173-183
Moore et al, Ann Surg 1992; 216: 173-183
Moore et al, Ann Surg 1992; 216: 173-183
Moore et al, Ann Surg 1992; 216: 173-183
Reynolds et al, JPEN; 21: 196-201
Reynolds et al, JPEN; 21: 196-201
Reynolds et al, JPEN; 21: 196-201
The Gut-Liver-TPN axis
• Promote gut function to diminish liver damage!!
–
–
–
–
–
–
•
•
•
Bacterial overgrowth etc
Bile acid pool (ursodeoxycholic acid)
Peristalsis and evacuation
Anatomy (blind loops, stenosis etc)
Infection/Inflammation
Nourish enterally as much as possible (Beware of
MOF, or abdominal infection)
Obesity, Diabetes, Alcohol riskfactors
Promote fat clearance (good fat, EN)
Promote EN to have fewer septic complications in
the short term??
The Relevance of intact
gutfunction
•
•
•
The Gut-Liver axis
Permeability and Translocation/MOF
Conclusions
Harris et al
Int Care Med
1992 18:38-41
Marshall et al Ann Surg 1993 218: 111-9
Sedman et al,
GE 1994
107: 643-9
Welsh et al
Gut 1998 42: 396-401
In addition: no correlation cultured microorganism at
operation and cause of sepsis
MOF via the gut
•
•
•
•
•
•
•
Meningococci sepsis insidious
Pneumococci sepsis insidious
Cholesepsis insidious
Urosepsis insidious
No MOF in celiac disease
No MOF in Crohn’s disease
Infection in Necrotising Pancreatitis takes 1 to
more weeks
• We have bacteriaemias continually and from
several sites (brushing teeth, furunculosis,
intercourse, gut etc)
• MOF from gut no prerequisite; gut permeability
non-specific
The Relevance of intact
gutfunction
•
•
•
The Gut-Liver axis
Permeability and Translocation/MOF
Conclusions
Conclusions
• There is much more to gut permeability: Normal
functioning of the gut
–
–
–
–
–
No strictures
No bypassed segments
No bacterial overgrowth
Normal bile acid pool
Normal peristalsis and activation (food)
– Essential for normal absorption of food
and for healthy liver-gut axis
• Importance of permeability for MOF overstated
Conclusions I
• Continuous TH1 and TH2 activity
• Pro-inflammatory activity defends against
protein antigens
• Anti-inflammatory acivity tapers the
inflammatory respons
• M.Crohn dysbalance between TH1 and Th2
activity
Conclusions II
• Increased permeability during starvation
• Decreased sIGA activity, increased bacterial
adhesiveness
• Bacterial overgrowth
• Diminished entero-hepatic cycling
• Increased sensitivity of the liver to toxic
influences
• Translocation bacteria and MOF unclear
• Inflammatory response in the mucosa may affect
liverfunction, mediated by cytokines
• Permeability badly defined!
Similar Pathology
•
•
•
•
•
•
•
Short bowel syndrome
Jejuno-ileal bypass
Primary Sclerosing Cholangitis
Kwashiorkor
Parenteral Nutrition and Gut Starvation
Blind loops
Etc
The significance of Bowel
permeability
• Permeability
• Clinical applicability
– Disease
– Nutrition
• Permeability and Translocation/MOF
• The Gut-Liver axis
• Conclusions
De nuchtere darm
• Aanwijzingen voor toegenomen
permeabiliteit
• Aanwijzingen voor verminderde villus
hoogte
• Veranderingen in functie
– Verminderde secretie sIGA (Alverdy)
Kyiama et al
JPEN 1998 22: 276-279
Darm-Lever-Organisme as
•
•
•
•
•
Een nuchtere darm
Stase van darminhoud
Secundaire galzouten
Ondervoeding/ Depletie
Kleine galzout pool
Stase van darminhoud
• Rotting en bacteriele overgroei
• Waarom beinvloedt dit de lever?
• Wat zijn de consequenties voor het hele
organisme?
• Multiple orgaan falen?
Darm-Lever-Organisme as
•
•
•
•
•
Een nuchtere darm
Stase van darminhoud
Secundaire galzouten
Ondervoeding/ Depletie
Kleine galzout pool
Secundaire galzouten
• Cholestatische en niet-cholestatische
galzouten
• Hydroxylering van galzouten
• Toxische effecten op de lever
• (kleinere galzout pool)
Darm-Lever-Organisme as
•
•
•
•
•
Een nuchtere darm
Stase van darminhoud
Secundaire galzouten
Ondervoeding/ Depletie
Kleine galzout pool
Ondervoeding/ Depletie
• Maakt de lever meer gevoelig voor de
effecten van alcohol, sec. galzouten etc.
• Kwashiorkor gele lever, groot,
hongeroedeem, ontsteking etc
• Verminderde functies van de darm
Welsh et al
Gut 1998 42: 396-401
Welsh et al
Gut 1998 42: 396-401
Darm-Lever-Organisme as
•
•
•
•
•
Een nuchtere darm
Stase van darminhoud
Secundaire galzouten
Ondervoeding/ Depletie
Kleine galzout pool
Kleine galzout pool
• Lever gevoeliger voor toxische invloeden
• Ondanks kleine galzout pool en snelle
passage toch vorming van sec. galzouten
(neonaten)
Evans et al
Br J Surg 1982 69: 706-8
Hongeren en metabole functie
van de darm
• Glutamine effecten
• Glutathion
• Labiele eiwit pool
Van der Hulst
Lancet 1993 334: 1363-5
Conclusies
• Relevantie darm-lever as duidelijk
• MOF onduidelijk
• Principe
– Kortgesloten darmgedeelten
– Extrahepatische cholestase/Hepatitis
– Primair scleroserende cholangitis/
inflammatoire darm ziekten
– Sepsis (Pneumonie biliaire)
– Jejuno-ileal bypass, Necrotiserende EnteroColitis/Lever (transplantatie)
Bondar et al
Arch Surg 1967 94: 707-16
Bondar et al
Arch Surg 1967 94: 707-16
Drenick et al
Gastroenterology 1982 82: 535-48
Merritt RJ
J Pediatric Gastroenterology Nutrition 1986 5: 9-22
Het jonge stel
Perdue Mary Am J Phys
1999 G1-G5
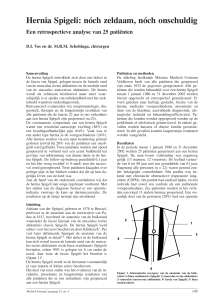
Nutritional depletion
Weight change with time in patients
with unresectable pancreatic cancer given EPA enriched supplement
35
30
Supplement
started
25
20
Weight
change 15
(kg)
10
5
0
-5
-10
-8
-6
-4
-2
0
Time (months)
M.D. Barber et al. ESPEN Nice 1998
2
4
6
8
10
Darm-Lever-Organisme as
• Wonderbaarlijk, dat een cellaag al de junk
buiten houdt
• Continue TH1 en TH2 activiteit
• Pro-inflammatoire activiteit maakt antigene
eiwitten onschadelijk
• Anti-inflammatoire aciviteit tapert de
ontstekingsreactie
• M.Crohn dysbalans tussen TH1 en Th2
activiteit
Kyiama et al
JPEN 1998 22: 276-279
Kyiama et al
JPEN 1998 22: 276-279
Bondar et al
Arch Surg 1967 94: 707-16
Travis et al Cl Science 1992: 82,471-88
Travis et al Cl Science 1992: 82,471-88
Bjarnason et al
GE 1995 108:1566-1581
Wyatt et al Lancet 1993 341:1437-39
Harris et al
Int Care Med
1992 18:38-41
Parks et al Br J of Surg 1996 83:1345-49
Parks et al Br J of Surg 1996 83:1345-49
Parks et al Br J of Surg
1996 83:1345-49
Drenick et al
GE1982 82:535-48
Drenick et al
GE1982 82:535-48
Garcia-Lafuente et al Gut 2001 48:503-507
Garcia-Lafuente et al Gut 2001 48:503-507
Gitter et al GE 2001 121:1320-28
Rocha et al Surgery 2001 130:65-73
Bjarnason et al
GE 1995 108:1566-1581