24-06-12
Diabetes = 90% Zelf-­‐management De beleving van de patiënt – soms somber, vol
weerstand, ontkennend. Hoe gaan we ermee
om?
Prof.dr Frank Snoek
Medische Psychologie/Diabetescentrum
VUMC
Amsterdam
[email protected]
Een diabetes patient staat gemiddeld per
jaar 6
uur in contact met zijn zorgverlener,
waarmee hij 8754 uren op zichzelf is
aangewezen….
www.diabetesmentaal.nl
www.diabetespsychology.nl
www.diabetergestemd.nl
Determinanten van Gedrag
Complexe interactie
• Overtuigingen (cognities)
• Emoties
Psychologie
(stress, gedrag)
Diabetes
(regulatie)
• Sociale context
Diabetes is psychisch belastend
• Diabetes is er altijd: zelf-regulatie 365 dagen-per-jaar
(“baan”)
• ‘Je best doen’ loont niet altijd; frustraties, boosheid
• Acute ontregeling (hyper, hypo) hinderlijk,
beangstigend, schaamtevol
• Wisselwerking stress-ontregeling
• Omgaan met (dreiging van) complicaties
• Sociale discriminatie, ‘negatieve’ steun (‘miscarried
helping’, ‘diabetes police)
Casus 1
Mevr. Van Nunen, 57 jaar
“ Type 2 diabetes, HbA1c 7.7% (was 6.7%), BMI 30,
somber, moeheidsklachten. Recent overlijden broer
met diabetes.
Steeds
meer moeite met zelfzorg”
Depressie,
verwerkingsproblematiek
Rubin, Peyrot,2001;Polonsky, 1999;
Jacobson, 1996 , Snoek ,2000
1
24-06-12
Diabetes ‘burnout’
Casus 2
Negatieve
ervaringen
Hr. Voorthuizen, 62 jaar
Diabetes-distress,
“ Type
2 diabetes, HbA1c somberheidsklachten
6,7%, Insuline,
Onzeker/afhankelijk
Hypoglykemieen,
stressklachten, slaapproblemen,”.
“Diabetes is een ramp.
Het zal me nooit
lukken!”
Negatieve
Attitude,
overtuigingen
Negatieve
emoties
‘Opgeven’
Matige zelf-zorg
Hoover JW, 1988; Polonsky WH, 1999; Seligman, 1997;
Snoek, 2000.
Problemen en Stoornissen
ANGST STOORNISSEN
- Gegeneneraliseerde Angststoornis en Fobieën
Coping/Aanpassingsproblemen
• Diabetes-distress/’burn out
• Sociale problematiek
Stoornissen (DSM-IV; ICD-10)
• Angststoornissen
• Eetstoornissen (AN, BN, Vreetbuien)
• Depressie (minor en major)
- Diabetes-specifiek:
• Spuit -/prik angst
• Angst voor hypoglykemie
Rubin, Peyrot, 2001; Snoek, Skinner, 2002;
Rubin, 2004
Angst voor Spuiten/Zelf-controleren (prikken)
• Prevalentie onder insuline-behandelde
patienten: 0.3 -1.0 %
• In 40% van de gevallen Spuitangst èn
Prikangst
• Lang niet altijd besproken met arts
• Fobische SA/PA gaat vaak samen met
depressie en/of andere fobieën
• Hoog HBA1c
Angst voor Hypoglykemie
• Prevalentie 5 -25% onder insuline-behandelde
patienten
• Risico verhoogd bij hypoglykemie ‘unawareness’
• Angstige patiënten (trait anxiety)
• Hypo-angst vertaalt zich in vermijdingsgedrag,
zowel actief als passief à Hoog HbA1c à
schuldgevoelens enz.
Mollema et al., 2001; Popkin et al, 1988
Gonder-Frederick et al., 1997; Marrero et al., 1997
2
24-06-12
Eetstoornissen
DEPRESSIE
• ‘Diaboulima’: Verhoogde prevalentie van (subklinische) Eetstoonissen - Boulimia Nervosa en
NAO bij Type 1 diabetes (meisjes)
• Onderdosering insuline (compensatoir gedrag)
komt bij 20% voor
• Vreetbuien (binge eating disorder) prevalent
bij Type 2 diabetes
• Anorexia Nervosa: verhoogde morbiditeit en
mortaliteit
Fairburn et al., 1991;Peveler et al, 1992; Rydall et al., 1997; Cow
et al., 2001; Neumark-Sztainer et al., 2002
Is Diabetes a risk factors for depression?
DEPRESSIE: Tweemal hogere prevalentie bij
diabetes
?
Depressie
Diabetes
Anderson RJ, et al. Diabetes Care. 2001;24(6):1069-­‐1078. Depressie is risicofactor voor diabetes Thomas Willis 1625-­‐1675: “Diabetes is a consequence of prolonged sorrow” H. Maudsley
"Diabetes is a disease which often
shows itself in families in which insanity
prevails….”
(The Pathology of Mind, 1899)
Knol MJ, et al. Diabetologia. 2006;49(5):837-­‐845. 3
24-06-12
Oorzaak verhoogde depressie bij
diabetes?
• Mensen met somaUsche chronische aandoening hebben overall 1.5 x meer kans een psychische stoornis te ontwikkelen • Psychosociale last van de diabetes (‘hardship
hypothese’)
• Biologische factoren: imflammatie (cytokines), neurohormonaal (HPA-as, cortisol)
Trimbos Instituut, 2006
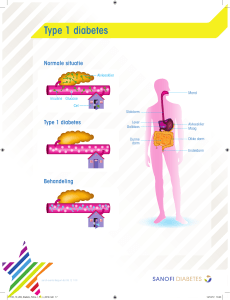
Depressie en Quality of Life bij diabetes Neither
DM only
Depression only
Depressie en incidentie diabetescomplicaties
: 5-jaars follow up
DM and Depression
100
Score
75
50
25
0
General
Health
Vitality
Mental
health
Physical
function
Goldney RD, et al. Diabetes Care. 2004;27(5):1066-1070.
Therapie ontrouw medicijnen en
Depressie
Social
Function
Microvasculaire complicaUes Macrovasculaire complicaUes Lin et al., Diabetes Care, 2010, 33,264-­‐269 Kosten: comorbide Depressie bij Diabetes 4000
Cost USD$
3000
2000
Mild depression
Moderate depression
Severe depression
1000
0
Adjusted model
Katon W, et al. Psychosomatic Medicine,2009,965-972
Ciechanowski et al. 2000, Arch. Intern. Med.
4
24-06-12
Richtlijn Depessie Screening in
ontwikkeling (NDF)
Matige herkenning depressie door
diabetes professionals
• Depressie gemist door medische professionals
30-50% (Valenstein, 2001; McDonald, 2002,
Lustman, 1987)
• Ook bij diabetesverpleegkundige
onderherkenning en registratie van angst/
depressie en diabetes-distress (max. 30%
herkend) (Pouwer, 2005)
• Screenen op depressie aanbevolen
(IDF,ADA,NDF)
• Standaard jaarlijks onderdeel jaarcontrole
• Gevalideerde screener (CES-D, PHQ-9, HADS,
WHO-5)
• Op indicatie nader onderzoeken
• Bespreken uitkomsten en koppelen aan zorgpad
• ‘ Matched’ care (passend hulp koppelen aan ernst/
zorgbehoefte)
Helpt depressie screening?
Screeners Depressie
• In eerstelijn helpt screening om herkenning te vergroten, en is
waarschijnlijk kosten-effectief (mits gevolgd door adequate zorg)
(Wells et al., 2000; Valenstein et al., 2001; Tylee, 2006; Barbui &
Tansella, 2006)
• CES-D (20 items)
• PHQ-9 (9 items)
• WHO-5 (5 items)
• Depressie screening met zorgpad op diabetespolikiniek
vermindert lijdensdruk en kosten (Simon et al., 2007)
• Geen diagnose maar waarschijnlijkheid (risico)
Monitor Depressie en Diabetes-Distress
• Monitoren en bespreken psychisch welbevinden als onderdeel
periodieke poliklinische diabetescontrole geeft significante
verbetering welbevinden en satisfactie met zorg
(Pouwer et al., 2001, De Wit, 2007; Snoek 2011, 2012 in press)
Rapport
MIND
2
kopieen
Depressie
D&
DD
DiabetesDistress
7-10 minuten
Actie/
verwijzing
Bespreking (15 min.)
5
24-06-12
Stapsgewijze behandeling
Ernstige
depressie
Milde depressie
Geen aanwijzingen voor
depressie
Behandeling depressie bij diabetes effectief
kleine effect size voor anti-depressiva:
d = -0.47 (95%CI -0.67;-0.27, N = 281)
Verwijzing,
psychotherapie,
pillen
Afwachten,
Counseling,
zelfhulp, psychoeducatie
gemiddelde effect size voor psychotherapie:
d = -0.58 (95%CI -0.77;-0.39, N = 310)
MA Van der Feltz-Cornelis 10
Internet (e-­‐mental health) ? DC voorlichting 21.11.11
Clinical Care/Education/Nutrition/Psychosocial Research
O R I G I N A L
A R T I C L E
Web-Based Depression Treatment for
Type 1 and Type 2 Diabetic Patients
A randomized, controlled trial
KIM M.P. VAN BASTELAAR,
FRANÇOIS POUWER, PHD3
PIM CUIJPERS, PHD2,4
MSC
1,2
HELEEN RIPER, PHD5
FRANK J. SNOEK, PHD1,2
OBJECTIVE—Comorbid depression is common in patients with type 1 and type 2 diabetes,
adversely affecting quality of life, diabetes outcomes, and mortality. Depression can be effectively
treated with cognitive behavior therapy (CBT). The Internet is a new and attractive method for
delivering CBT intervention on a large scale at relatively low costs. This study evaluated the
effectiveness of Web-based CBT for depression treatment in adults with type 1 or type 2 diabetes,
with minimal guidance.
RESEARCH DESIGN AND METHODS—A randomized controlled trial was conducted
in the Netherlands in 255 adult diabetic patients with elevated depressive symptoms. Primary
outcomes were depressive symptoms. Secondary outcomes were diabetes-specific emotional
distress and glycemic control. Assessments were at baseline, after treatment, and at the 1-month
follow-up.
RESULTS—The Web-based CBT was effective in reducing depressive symptoms by intentionto-treat analyses (P = 0.04, d = 0.29; clinical improvement 41% vs. 24% P , 0.001) and by perprotocol analyses (P , 0.001, d = 0.70; clinical improvement, 56% vs. 24% P , 0.001). The
intervention reduced diabetes-specific emotional distress (P = 0.03) but had no beneficial effect
on glycemic control (P . 0.05).
CONCLUSIONS—Web-based CBT depression treatment is effective in reducing depressive
symptoms in adults with type 1 and type 2 diabetes. In addition, the intervention reduces diabetes-specific emotional distress in depressed patients.
Diabetes Care 34:320–325, 2011
A
ffecting 10 to 20% of adult diabetic
patients, depression is a common
comorbid health problem among
people with type 1 or type 2 diabetes
(1). Comorbid depression in diabetes results in a lower quality of life, poorer glycemic control, an increased risk of
developing diabetes-related complications, and higher mortality rates (2). Depression, therefore, needs to be regarded a
serious and common comorbidity in diabetes, negatively affecting both mental
and physical health.
In routine diabetes care, depression
remains untreated in at least 50% of the
patients (2). Undertreatment occurs
partly because patients are not inclined
to discuss their emotional problems
with their physician, and health care professionals feel under-resourced and lack
the tools to refer or treat depression in
their diabetic patients (2).
A recent meta-analysis showed that
depression in people with diabetes can be
treated effectively with antidepressant
medication, psychotherapy, or combined
c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c
From the 1Department of Medical Psychology, VU University Medical Center, Amsterdam, the Netherlands;
the 2Institute for Health and Care Research (EMGO Institute), VU University Medical Center, Amsterdam,
the Netherlands; the 3Department of Medical Psychology & Neuropsychology, Center of Research on
Psychology in Somatic diseases (CoRPS), Tilburg University, Tilburg, the Netherlands; the 4Department of
Clinical Psychology, VU University, Amsterdam, the Netherlands; and the 5Netherlands Institute of Mental
Health and Addiction (Trimbos), Utrecht, the Netherlands.
Corresponding author: Kim M.P. van Bastelaar, [email protected].
Received 1 July 2010 and accepted 22 October 2010.
DOI: 10.2337/dc10-1248. Clinical trial reg. no. ISRCTN24874457, isrctn.org.
© 2011 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and the work is not altered. See http://creativecommons.org/
licenses/by-nc-nd/3.0/ for details.
320
DIABETES CARE, VOLUME 34, FEBRUARY 2011
therapy, with possible benefits on diabetes
outcomes (3). A meta-analysis showed that
using the Internet to deliver psychotherapy
is an effective treatment option for depression and could help to increase reach and
facilitate access to effective depression
treatment against relatively low costs (4).
Lewinsohn’s Coping with Depression
course (CWD) is currently the most
studied and proven effective cognitive behavioral therapy (CBT) treatment of depression, and given its highly structured
character, is suitable for making a Webbased version (5). The effectiveness of a
Web-based version of CWD—Color Your
Life (CYL)—has been shown (6,7). Because CWD, and specifically CYL, is
highly structured, it requires adaptation
to subgroups of patients that are being
addressed, such as those previously developed and tested in randomized controlled trials in elderly, young people,
and patients with chronic diseases (5).
Between 56 and 75% of depressed
patients with diabetes experience high
levels of emotional distress directly related to diabetes (8). Recent studies have
shown that the beneficial effects of depression treatment on glycemic control
are mediated by diabetes-related distress
(9,10). Health care providers have therefore been advised to address diseasespecific emotional distress to improve
the effectiveness of depression treatment
and to benefit diabetes outcomes (9).
Therefore, in close collaboration with
the researchers who developed CYL, we
adapted this course to meet the needs of
diabetic patients, thus maximizing acceptability (11). This diabetes-sensitive
CYL (Diabetergestemd.nl, DG.nl) takes
into account the specific coping issues
diabetic patients are faced with related to
physical problems, the daily burden of selfmanagement, and the risk of long-term
complications. The need to adapt CWD to
diabetic patients was confirmed by consulting diabetic patients, professionals, and from
our own clinical experience (11).
The primary aim of this study was to
test the effectiveness of DG.nl in a randomized controlled trial. We hypothesized that depressive symptoms would
care.diabetesjournals.org
6
24-06-12
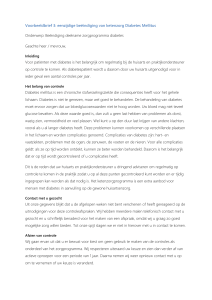
Klinisch relevante verandering (verschil
tussen groepen)
Recovered (CES-D < 16) & improved (RC-index: CES-D -5) at one month follow-up
Secondaire Analyses: worden uitkomsten
gemodificeerd door klinische ernst?
• Effectiviteit Diabetergestemd.nl niet anders
voor patienten met milder vs. ernstiger profiel
Intention to treat analysis
41% <0.001
CBT
Waiting list
24%
Per protocol analysis
56%
CBT
Waiting list
<0.001
24%
Van Bastelaar JMIR, 2012
Psychologisch Hulpaanbod?
• Luisterend oor, oog voor de psychosociale dimensie
• Ondersteunende gesprekken (counseling)
• Groepscursussen (mindfullness, omgaan met
chronische ziekte)
• Begeleide zelf-hulp: www.diabetergestemd.nl
• 1e lijns psycholoog, psychotherapeut, psychiater,
GGZ
• Gespecialiseerde Polikliniek Diabetes Mentaal
VUMC(www.diabetesmentaal.nl)
Altijd aandacht voor welzijn van de patiënt
Insuline: bitterzoet vooruitzicht ?
“
NO HEALTH WITHOUT
MENTAL HEALTH”
Hoe kunnen we barrières bij de overgang naar
insulinetherapie slechten ?
Langerhans 2012
Yvonne Woudenberg, MSc
praktijkverpleegkundige/epidemioloog
Prince et al., Lancet, 2007
7
24-06-12
filmpje allochtonen en diabetes
Meet Mr. Jones
Psychologische insulineresistentie
• Brits onderzoek 2007
• 2500 type 2 diabeten
• HbA1c ≥ 8 % (≥ 64 mmol/mol) en max.
orale medicatie
• na 5 jaar 50 % aan insuline
Rubino et al, DiabeUc Medicine 2007 Psychologische insulineresistentie
“Het is mijn eigen schuld, had ik me maar beter aan
mijn dieet gehouden”
“Wat zullen anderen wel niet denken als ze me zien
spuiten ? Ze denken vast dat ik een junkie ben”
“Insuline is slecht voor je. Ik ken iemand die blind werd
na het starten met insuline”
Psychologische insulineresistentie
•
•
•
•
1/3 van de insulinenaïeve type 2 diabeten
PIR wordt gemeten met ITAS 1
ITAS = Insuline Therapie Attitude Schaal
depressie, slechte algehele gezondheid,
hoge stress aangaande diabetes en
laaggeschoold 2
1 Snoek et al, Health Qual Life Outcomes 2007 2 Larkin et al, Diabetes Educator 2008 Makine et al, DiabeUc Medicine2009 8
24-06-12
PIR in huisartsenpraktijk
• depressie
• levenslang insuline
Levenslang insuline
• plezierige activiteiten opgeven
• moeilijker verantwoordelijkheden te dragen
(op het werk, thuis)
• afhankelijker van dokter
Woudenberg, Lucas, Latour, Scholte op Reimer, DiabeUc Medicine 2011 Woudenberg, Lucas, Latour, Scholte op Reimer, DiabeUc Medicine 2011 Praktijk
Praktijk
Afgeschermde naald
• benadrukken dat insuline normale, verwachte stap is • weigeren insuline betekent niet dat geleverde zorg wordt verminderd • bespreek reeds bekende hypoklachten • benoem voordelen normoglycemie op korte termijn Autocover
Autoshield
9
24-06-12
Eerste keer samen prikken
Even proberen
Praktijk Praktijk
• psycholoog
• biedt wijkverpleging aan voor opstartfase
10