HIV-infectie en NASH
C.Richter
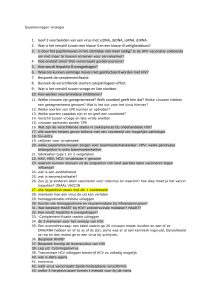
Liver disease in HIV:
raised aminotransferases
HCV or HBV
Immune
Restoration
Disease
Direct
Cytotoxicity
Chronic
Hepatitis
Alcohol
Drugs
Drug-related
Hepatotoxicity
Medications
NASH
HIV
HAART
Drug induced hepatotoxicity
Frequency of drug induced
hepatotoxicity
• Nevirapine : 4-18% (contraindications:
CD4>250 in women and >400 in men!
• Efavirenz: 1-9%
• Abacavir (hypersensitivity)
• DDI/D4T: Lactic Acidosis
• DDI: non cirrhotic portal hypertension
• Protease inhibitors: 1-9.5%
Microvesicular steatosis secondary
to HAART
Mechanisma of drug induced
hepatotoxicity in HIV patients
• Hypersensitivity reaction (nevirapine, efavirenz, abacavir
– not dose related)
• Idiosyncratic
• Mitochondrial toxixity (DDI/D4T*)
• Hepatic steatosis
• Immune reconstitution (HBV,HCV/CMV)
• *Neth J Med. 2000 Nov;57(5):190-3.
• Hepatic steatosis and lactic acidosis caused by
stavudine in an HIV-infected patient.
• Bleeker-Rovers CP, Kadir SW, van Leusen R, Richter C.
Risk factors for HIV-drug induced
hepatotoxicity
• Alcohol use
• Preexisting fibrosis/cirrosis
• Co-infections with HBV/HCV
HIV-HBV/HCV coinfecties in SHM
cohort
• Ongeveer 13000 van 15000 getest voor zowel
HBV and HCV, 1100 getest voor alleen HBV en
340 uitsluitend voor HCV.
• 1149/14160 = 8% HbsAg
• 1609/13396 = 12% HCV
• Triple infectie HIV/HBV/HCV: 1%
• Hazard ratio voor dood met co-infectie:
HBV 1.54, HCV:2.3 (vgl met HIV)
SHM 2009
Invloed van HIV op Hep B en C
• HIV verhoogd de HBV- en HCV-replicatie
• HIV vergroot de kans op ontstaan van
lever-cirrose, leverfalen en HCC
• Maar: De invloed is minder bij stabiele
HIV-infectie met neg.HIV-RNA en redelijk
goede cellulaire immuniteit!
Verschil tussen Afrikaanse pat. met
HIV/HBV en Nederlandse patient
• Afrikaan van 30 jaar kan al 30 jaar
chronische hepatitis B hebben met
verhoogde kans op HCC en levercirrhose
• Nederlandse homoseksuele man van 30
jaar is bij presentatie nog niet bedreigd
door levercomplicaties
Wat heeft hepatitis B met Nash te
maken?
• Levercirrhose kan trigger zijn voor
ontstaan van DM, metabool syndroom
HIV/HBV Co-infection:
Effect on Liver-related Mortality
Liver-related mortality rate
(per 1000 person-years)
16
P<0.0001
14
12
10
8
6
4
P<0.001
P=0.04
2
0
HIV-/HBsAg-
HIV+
Thio CL, et al. 9th CROI; 2002; Seattle, Wash. Abstract 656.
lancet
HBsAg+
HIV+/HBsAg+
5
HCV en steatosis/ metabool
syndroom
• HCV veroorzaakt metabool syndroom
• 20% van pat. met milde baseline steatose en
fibrose:6 jaar later ernstige fibrose/steat
• Hoofdoorzaken:
- insuline resistentie (blokkade
intracellulaire insuline signalering)
- oxidative stress
- modificatie proinflammatoire cytokines
- downregulatie adinoponectin, upregulatie
leptin
Steatose in hepatitis C in relatie tot
genotype
Genotype 3a: meer kans op steatose dan bij
andere genotypes, reden??
Ontstaan van steatose (vet in >5%
hepatocyten)
- Toename lipide accumulatie in hepatocyten
- Verhoging vrije vetzuursynthese
- Verlaging lipide oxidatie en secretie
Behandeling hepatitis C in
aanwezigheid steatose en DM
• Meer kans op relaps, langere therapie!
• Eerst goede behandeling DM en metabool
syndroom voor start therapie voor hepatitis
C?
• Vroege behandeling hepatitis C om
ontstaan van DM, metabool syndroom en
fibrose/cirrose te voorkómen?
• Nieuwe ontwikkeling HCV therapie?
HCV therapie anno 2012
• Genotype 2/3: 70-80% SVR
• Hoofdprobleem is genotype 1 (50% in NL)
SVR (genezing)
- Naïef
- Relapser
- Partial responder
- Null responder
tot 2012
46%
22%
15%
5%
vanaf 2012
79%
86%
59%
15%
Kan over 10 jaar elke HCV patiënt
worden genezen?
• Waarschijnlijk wel!
• Nieuwe middelen tegen hepatitis C:
- 2. generatie protease remmers
- NS5A inhibitors
- polymerase remmers (nucleosides en
nucleotides)
- cyclophylin inhibitors
- peg-IFN – lamda (zeer effectief en veel
minder toxisch dan peg-IFN alfa)
Patients in the HAART era have at least a 10-year
shorter expected survival than age- and gendermatched controls
Survival from age 25 years (N=3,990)
Probability of survival
1
0.75
Population
controls
0.5
Late HAART
(2000–2005)
0.25
Early HAART
(1997–1999)
Pre-HAART
(1995–1996)
0
25
30
35
40
45
50
55
60
65
70
Age, years
Adapted from Lohse N, et al. Ann Intern Med 2007;146:87–95.
Causes of death of patients with
HIV disease
HAART is associated with reduced immune
activation, but levels remain high vs HIV-negative
subjects
CD8+
30
20
P<0.001
P<0.001
10
0
HIV infected HIV infected
HIV
untreated
treated
uninfected
(N=13)
(N=99)
(N=6)
Percentage of activated
CD8+ T cells
Percentage of activated
CD4+ T cells
CD4+
30
20
P<0.001
P<0.001
10
0
HIV infected HIV infected
HIV
untreated
treated
uninfected
(N=13)
(N=99)
(N=6)
Adapted from Hunt PW, et al. J Infect Dis 2003; 187:1534–1543.
Many biomarkers of immune activation, inflammation, and
endothelial activation have been identified
• These markers may provide additional prognostic
information on disease progression and treatment
Inflammation
Endothelial activation and damage
Coagulation
response
–Adiponectin • Soluble
–D-dimer
intercellular
adhesion molecule
–Amyloid P
and cell adhesion
–E-selectin
–Prothrombin
molecule
(sICAM–Amyloid A
fragment
–Granulocyte 1 and sVCAM-1)
• Tissue-type
–C-reactive
1+2 (F1.2)
plasminogen
activator (t-PA)
protein
macrophag
and activator
(CRP)
inhibitor (t-PAI-1)
e colonyWillebrand
–Interleukin 6 stimulating • von
factor (vWF)
(IL-6)
factor (GMKuller L, et al. 15th CROI 2008. Abstract 139. Ross A, et al. 15th CROI 2008; Abstract 949.
Ross A, et al. 15th CROI 2008; Abstract 954. Calmy A, et al. 15th CROI 2008; Abstract 140.
CSF)
–Tumor
necrosis
Patient A
• Diabetes mellitus sinds 1991
• HIV-infectie stadium C3, presentatie PJP
in 1998
• Op HAART sinds 1998, tijdelijk zonder
therapie voor diabetes
• Gewichtstoename met BMI 45,
buikomvang 120 cm, toenemende insuline
resistentie, voor ernstig OSAS: CPAP
Voortzetting patiënt A
•
•
•
•
•
•
HIV-RNA steeds negatief
CD4 prima: > 600
DM-2 matig ingesteld: Hba1c: 72 (8.8%)
ALF 151, y-GT 307, ASAT 57, ALAT 63
Echo lever: uitgebreide steatose
Leverbiopt:
Fibrosis Staging of Liver Biopsies
no fibrosis
extraportal fibrosis
portal fibrosis
bridging fibrosis
cirrhosis
Conclusie patiënt A
• Bridging fibrosis op basis van NASH
• Patient ws meer bedreigd door leverziekte
(voorstadium cirrhose) dan door HIV
• Hoe hadden wij het kunnen voorkómen?
• Vasulaire poli: Uitgebreide
leefstijladviezen hebben weinig effect
• Wat nu? gastric bypass?
Non alcoholic fatty liver disease in
HIV-infected patients
• Hogere prevalentie (30-40%) dan in algemene
bevolking (14-30%)
• Metabool syndroom neemt toe: van 19% in 2000
naar 42% in 2007
• Risk factoren gerelateerd aan HIV-infectie,
HAART en co-infectie hepatitis B/C
- verminderde glucose tolerantie, insuline
resistentie
- veranderd lipide metabolisme (laag HDL, hoog
triglyceride), lichaamsvet redistributie met
centrale adipositas
Wanneer moet men alert zijn op
NASH?
• Levermanifestatie van metabool syndroom
• Bij elke patiënt met M Syndroom eraan
denken (Divas zorg, obesitas poli)
• Bij elke patiënt met HIV-infectie en/of
hepatitis C (infectie-poli, MDL poli)
• Bij elke patiënt voor analyse
leverenzymstoornis (MDL,Interne)
Hoe kun je diagnose van NASH
stellen?
• Voldoen aan criteria metabool syndroom
• Afwijkende leverenzymen
- ALAT verhoogd? Cut-off 2x ULN
ws.niet zinvol
- Y-GT : sterke relatie met steatosis en bij HCV ook met fibrose
(onderschat parameter? (prospect. Belg.studie over associatiie
fibrosis/metabool syndroom, (S.Francque et al., acta
gastroenterolica belg 2011)
• Echo lever: hyperechogeniciteit : steatose
• Rol voor fibroscan: goed voor diagnostiek ernstige fibrose, maar
verstoort door inflammatie/adipositas
• Dus: leverbiopt bij welke combinatie van factoren?
Hoe kun je NASH behandelen?
• …..
• …..
• …..
Kun je NASH voorkómen?...
• …..
Samenvatting
• NASH bij HIV patiënten is multifactorieel
bepaald en ingewikkeld
• NASH zal de komende decennia
toenemen en verdient ook bij HIV
patiënten meer aandacht
• Het wordt tijd voor multidisciplinaire
samenwerking op gebied van NASH
Causes of liver disease of patients
with HIV-infection